The term enteric fever is used to describe acute infection caused by Salmonella typhi (typhoid fever) or Salmonella paratyphi (paratyphoid fever). Besides these 2 salmonellae, Salmonella typhimurium causes food poisoning.
PATHOGENESIS
The typhoid bacilli are ingested through contaminated food or water.
During the initial asymptomatic incubation period of about 2 weeks, the bacilli invade the lymphoid follicles and Peyer’s patches of the small intestine and proliferate.
Following this, the bacilli invade the blood-stream causing bacteraemia, and cause the characteristic clinical features of the disease like continuous rise in temperature and ‘rose spots’ on the skin.
Immunological reactions (Widal’s test) begin after about 10 days and peak titres are seen by the end of the third week.
Eventually, the bacilli are localised in the intestinal lymphoid tissue (producing typhoid intestinal lesions), in the mesenteric lymph nodes (leading to haemorrhagic lymphadenitis), in the liver (causing parenchymal necrosis), in the gallbladder (producing typhoid cholecystitis), and in the spleen (resulting in splenic hyperplasia).
MORPHOLOGIC FEATURES
The lesions are observed in the intestines as well as in other organs.
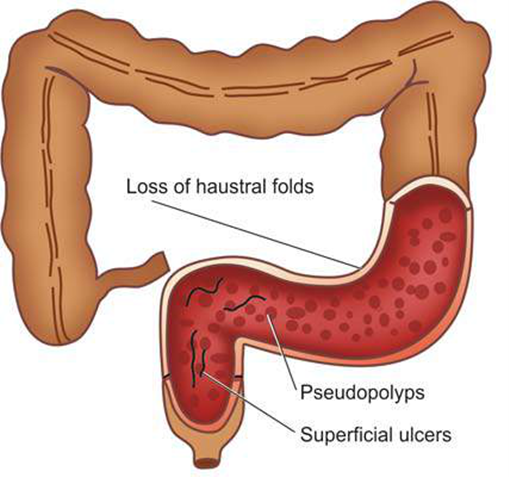
- INTESTINAL LESIONS
Terminal ileum is affected most often, but lesions may be seen in the jejunum and colon.
Peyer’s patches show oval typhoid ulcers with
The base of the ulcers is black due to sloughed mucosa.
The margins of the ulcers are slightly raised due to inflammatory oedema and cellular proliferation.
There is never significant fibrosis, and hence fibrous stenosis seldom occurs in healed typhoid lesions.
The regional lymph nodes are invariably enlarged.
Fig: Typhoid Intetstinal Ulcer
Microscopically, there is hyperemia, oedema and cellular proliferation consisting of phagocytic histiocytes (showing characteristic erythrophagocytosis), lymphocytes and plasma cells.
Though enteric fever is an example of acute inflammation, neutrophils are invariably absent from the cellular infiltrate, and this is reflected in the leukopenia with neutropenia and lymphocytosis.
The main complications of the intestinal lesions of typhoid are perforation of the ulcers and haemorrhage. - OTHER LESIONS
Besides the intestinal involvement, various other organs and tissues showing pathological changes in enteric fever are as under:
i) Mesenteric lymph nodes—haemorrhagic lymphadenitis.
ii) Liver—foci of parenchymal necrosis.
iii) Gallbladder—typhoid cholecystitis.
iv) Spleen— splenic hyperplasia
v) Kidneys—nephritis.
vi) Abdominal muscles—degeneration.
vii) Joints—arthritis. Etc.
Persistence of organism in the gallbladder or urinary tract may result in passage of organisms in the faeces or urine creating a ‘carrier state’ which is a source of infection to others.