Alzheimer’s disease is the most common cause of dementia in the elderly.
The disease usually becomes apparent as gradual impairment of intellectual function, with alterations in mood and behaviour.
Later, progressive disorientation, memory loss, and aphasia occur, indicating severe cortical dysfunction.
Etiopathogenesis
The exact cause is not known, but a few factors are involved in its etiology, which includes-
- Positive family history.
- Down’s Syndrome
- Point mutations in APP coding gene
- Deposition of Ab amyloid that forms plaques.
- Deposition of tau protein that forms neurofibrillary tangles
In Alzheimer’s disease accumulation of two proteins amyloid and tau takes place in specific brain regions because of excessive production and defective removal. Two pathologic hallmarks of AD are amyloid plaques and neurofibrillary tangles.
Plaques are deposits of aggregated Ab peptides while tangles are aggregates of microtubule binding protein tau.
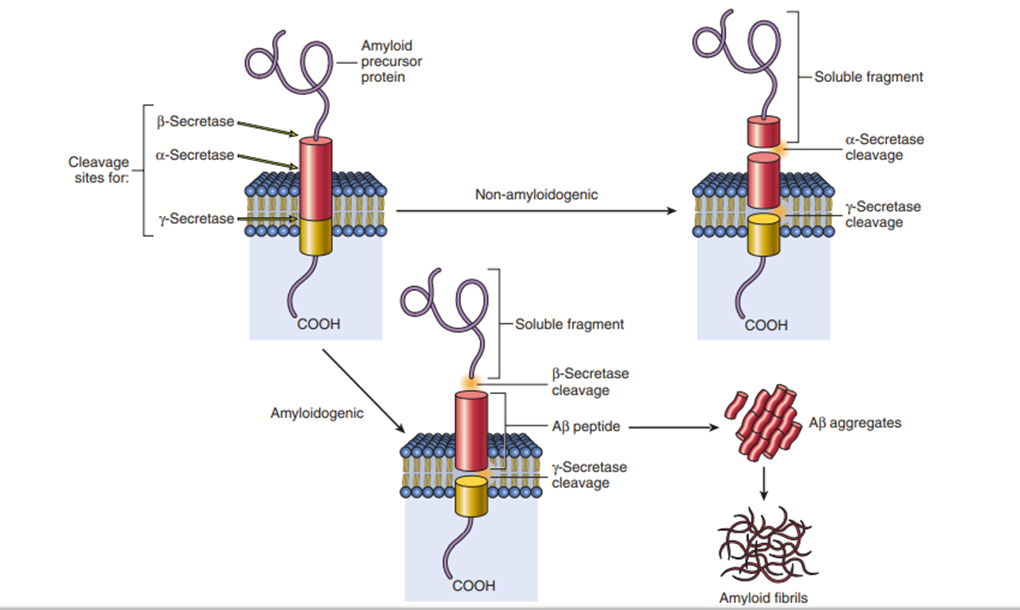
Aβ Generation
The fundamental abnormality in AD is the deposition of Aβ peptides that occur due to improper processing of APP (Amyloid precursor protein).
APP is a cell surface protein having a single transmembrane domain that functions as a receptor. The Aβ portion of the protein extends from the extracellular region into the transmembrane domain.
Processing of APP begins with cleavage of APP domains.
If the first cut occurs at the α-secretase site followed by cleavage at γ-secretase sites, a soluble fragment is formed, and Aβ will not be generated (the nonamyloidogenic pathway).
But if the first cut occurs at the β-secretase site followed by cleavage at γ-secretase sites, then then Aβ will be generated.
Once generated, Aβ aggregates first into small oligomers and eventually forms large aggregates and fibrils. These aggregates are neurotoxic. Aggregates of Aβ can result in synaptic dysfunction. These aggregates elicit an inflammatory response from microglia and astrocytes. These inflammatory cascades may cause alterations in tau phosphorylation, along with oxidative injury to the neurons.
Neurofibrillary Tangles
Neurofibrillary tangles contain the tau protein. Tau is a microtubule-binding protein. With the development of tangles in AD, it becomes hyperphosphorylated, and loses the ability to bind to microtubules.
Both plaques and tangles contribute to neuronal dysfunction.
Morphological features
- The brain is often reduced in weight and atrophic.
- Senile neuritic plaque containing Ab amyloid.
- Neurofibrillary tangle is a filamentous collection of neurofilaments and neurotubules within the cytoplasm of neurons due to dysfunctional microtubule binding protein tau.
Clinical features
Initial stages- forgetfulness, memory disturbances
Progressive stages- language difficulty, loss of mathematical skills, and loss of motor skills.
Final stages- Patient becomes mute, problem in movements and walking, severe dementia, lack of facial expression.