Pathologic or heterotopic calcification is the abnormal tissue deposition (in tissues other than (osteoid or enamel) of calcium salts, together with smaller amounts of iron, magnesium, and other mineral salts.
There are two forms of pathologic calcification.
Dystrophic Calcification– Dystrophic calcification is characterised by deposition of calcium salts in dead or degenerated tissues with normal calcium metabolism and normal serum calcium level.
Metastatic calcification – In contrast, the deposition of calcium salts in otherwise normal tissues is known as metastatic calcification, and it mostly results from hypercalcemia and some disturbance in calcium metabolism.
Dystrophic Calcification
Causes:
- Dystrophic calcification is encountered in areas of different types of necrosis (of coagulative, caseous, or liquefactive type)
- Foci of enzymatic necrosis of fat.
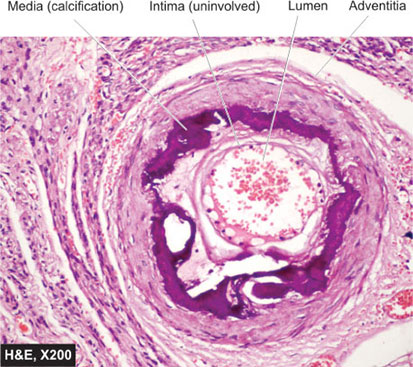
- Calcification is mostly present in the atheromas of advanced atherosclerosis.
- Calcification commonly develops in aging or damaged heart valves, further hampering their function.
- Cysts which have been present for a long time may show calcification of their walls e.g., epidermal and pilar cysts.
*→Although dystrophic calcification may simply be a sign of previous cell injury, it is often a cause of organ dysfunction. This is the case in calcific valvular disease and atherosclerosis.
→Serum calcium level is normal in dystrophic calcification.
Metastatic calcification
Metastatic calcification may occur in normal tissues due to hypercalcemia.
Causes: There are four principal causes of hypercalcemia:
- increased secretion of parathyroid hormone (PTH) with subsequent bone resorption, as in hyperparathyroidism due to parathyroid tumors, and abnormal secretion of PTH-related protein by malignant tumors
- →resorption of bone tissue
→tumours of bone marrow (e.g., multiple myeloma, leukemia) or →diffuse skeletal metastasis (e.g., breast cancer),
→accelerated bone turnover (e.g., Paget disease),
→Prolonged immobilisation of a patient results in disuse
atrophy of the bones and hypercalcaemia.
- Vitamin D–related disorders-
→vitamin D intoxication
→sarcoidosis
→idiopathic hypercalcemia of infancy (Williams syndrome), characterized by abnormal sensitivity to vitamin D
- Renal failure, which causes retention of phosphate, leading to secondary hyperparathyroidism.
Less common causes-
- Aluminium intoxication, which occurs in patients on chronic renal dialysis.
- Milk-alkali syndrome caused by excessive oral intake of
calcium in the form of milk and administration of calcium
carbonate in the treatment of peptic ulcer.
Sites of metastatic calcification- Metastatic calcification may occur widely throughout the body but principally affects the interstitial tissues of the gastric mucosa, kidneys, lungs, systemic arteries, and pulmonary veins. Although quite different in location, all these tissues excrete acid and therefore have an internal alkaline compartment that predisposes them to metastatic calcification.
Calcium salts may occur as noncrystalline amorphous deposits or as hydroxyapatite crystals. Usually, the mineral salts cause no clinical dysfunction, but massive involvement of the lungs produces remarkable x-ray images and respiratory compromise. Massive deposits in the kidney (nephrocalcinosis) may cause renal damage.
REFERENCE
Harsh Mohan; Text book of Pathology; 6 th edition; India; Jaypee Publications; 2010